在2016年中原心脏病学大会中,来自复旦大学附属中山医院的周京敏教授带来了题为“心衰患者的容量管理”的精彩报告

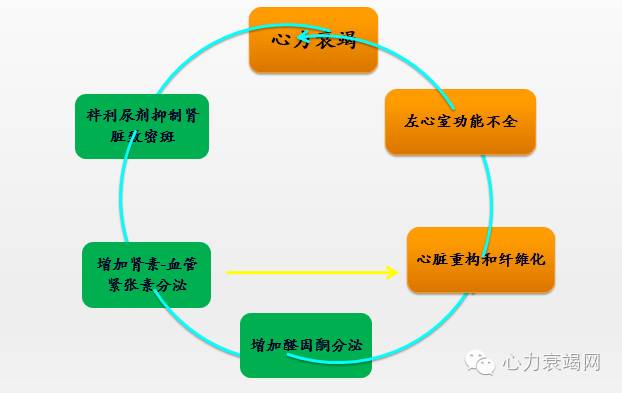
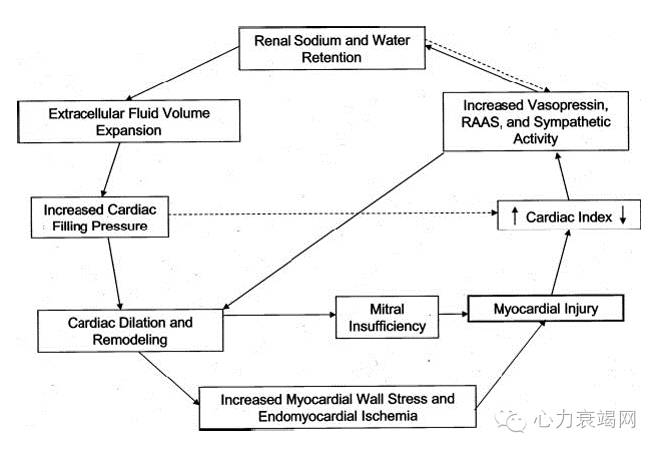
心衰容量负荷增加与多种机制有关
1.慢性HF-REF(NYHA Ⅱ-IV级)处理流程
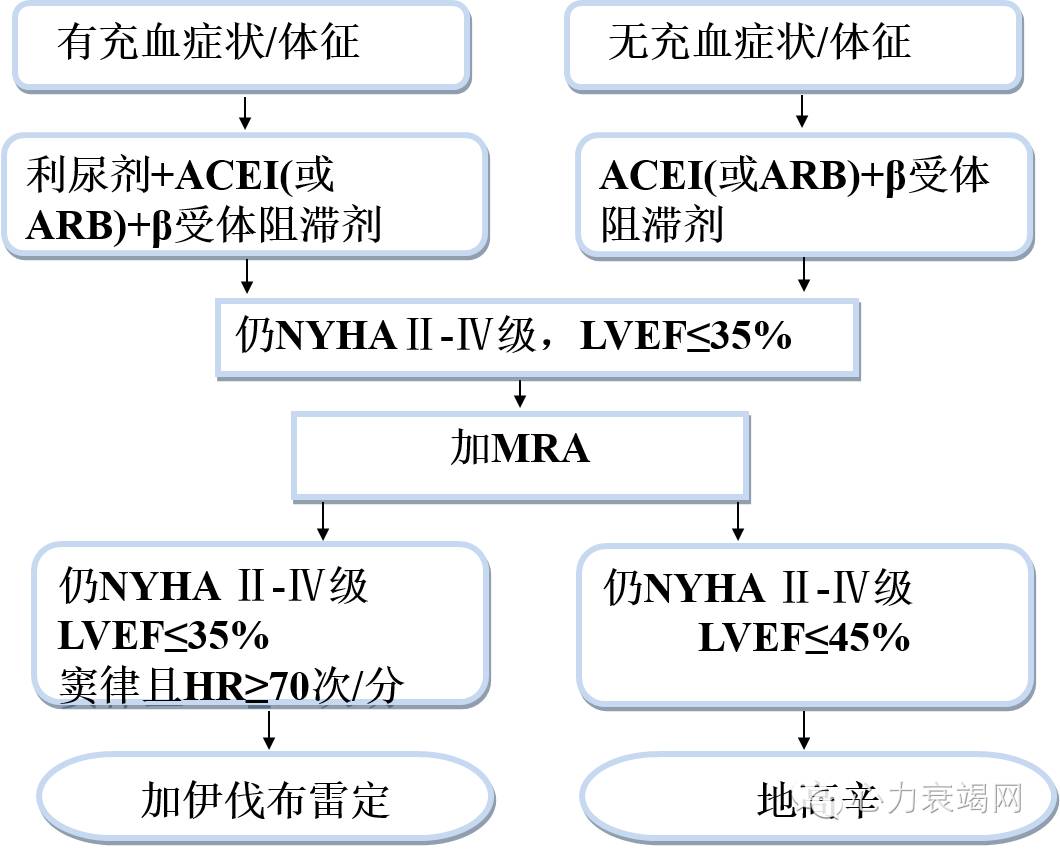
容量负荷过重:最重要、最基础的改变
2.容量超负荷的后果
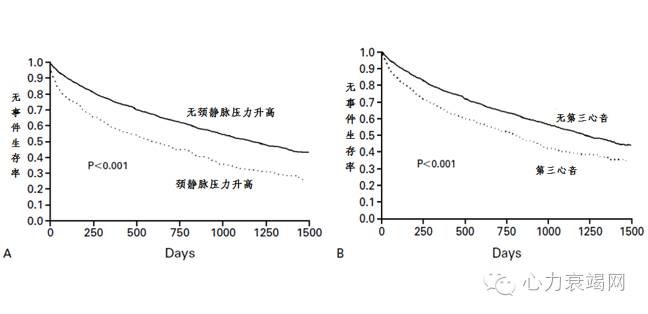
3.体液潴留使患者预后恶化
[1]
4.心衰患者住院前30天体重开始增加
[2]
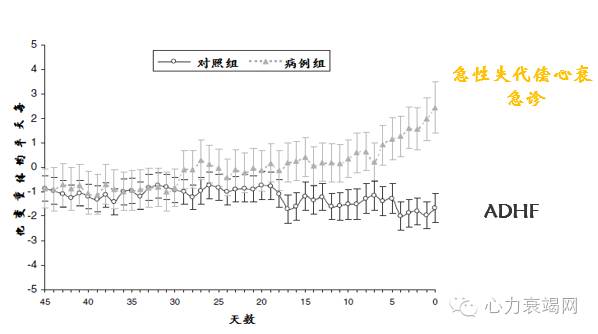
研究显示:患者在住院前30天起,体重就开始慢慢逐步增加
5.欧洲心衰充血评分
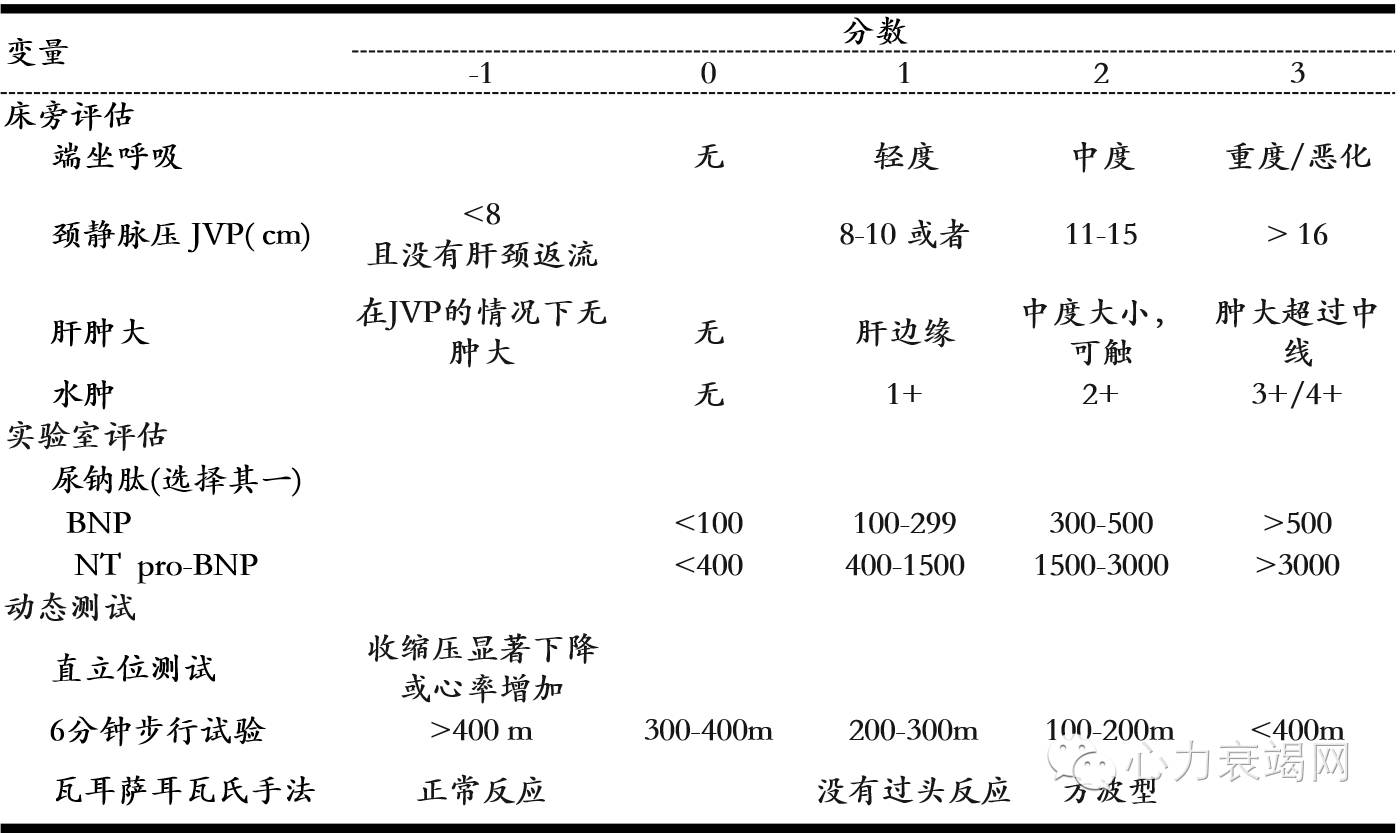
所以正确评估并分级急性心衰患者的充血状况非常重要
欧洲心血管协会心力衰竭委员会暨欧洲危重监护医学协会2010发表《急性心衰的评判共识》
不仅包括临床充血,也包括临床充血和血流动力学充血
可选择的治疗策略
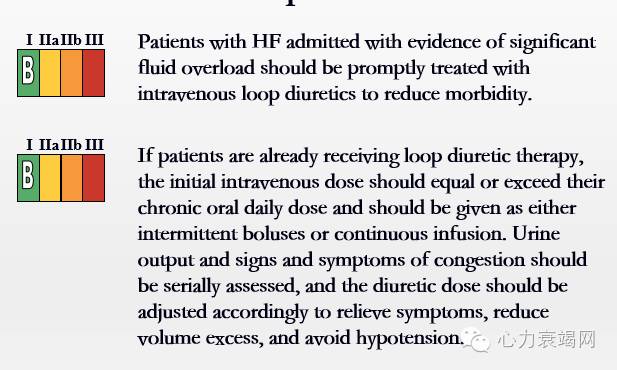
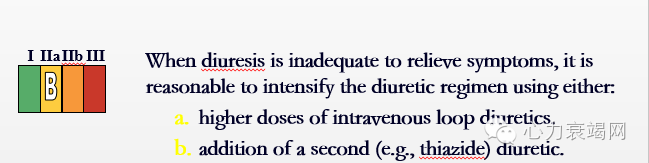
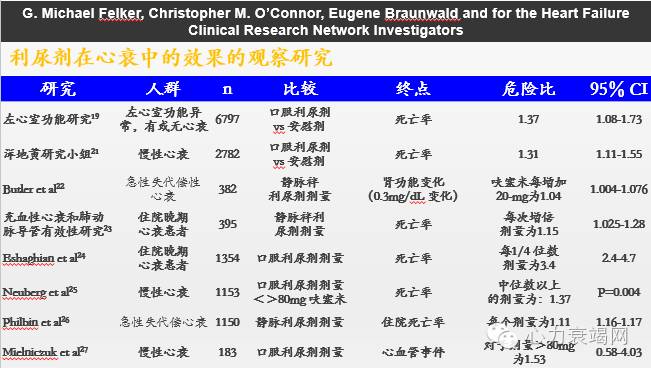
1、利尿剂: Diuretics in Hospitalized Patients
Diuretics in Hospitalized Patients
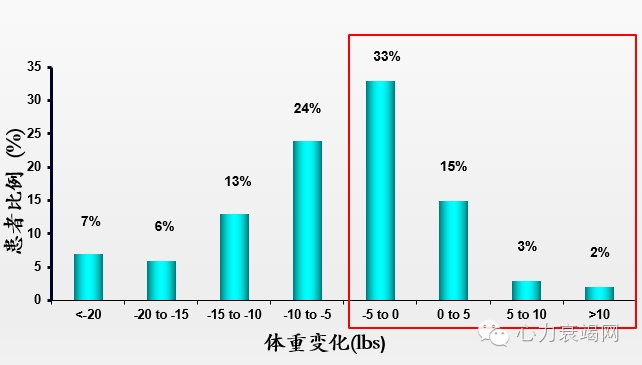
大多数患者体重没有或只有轻微下降
[3]
尽管体液潴留,或称充血是心衰患者住院的主要原因,美国 急性失代偿性心力衰竭全国注册研究(The Acute Decompensated HEart Failure National REgistry (ADHERE(tm))显示L将近50%的患者住院期间其中没有或者只有微小变化. . N=96,094
Although congestion is the main reason for heart failure hospitalizations, the ADHERE Registry data showed that close to 50% of patients have minimal or no weight loss during their hospital stay. N=96,094
袢利尿剂对RAAS系统影响
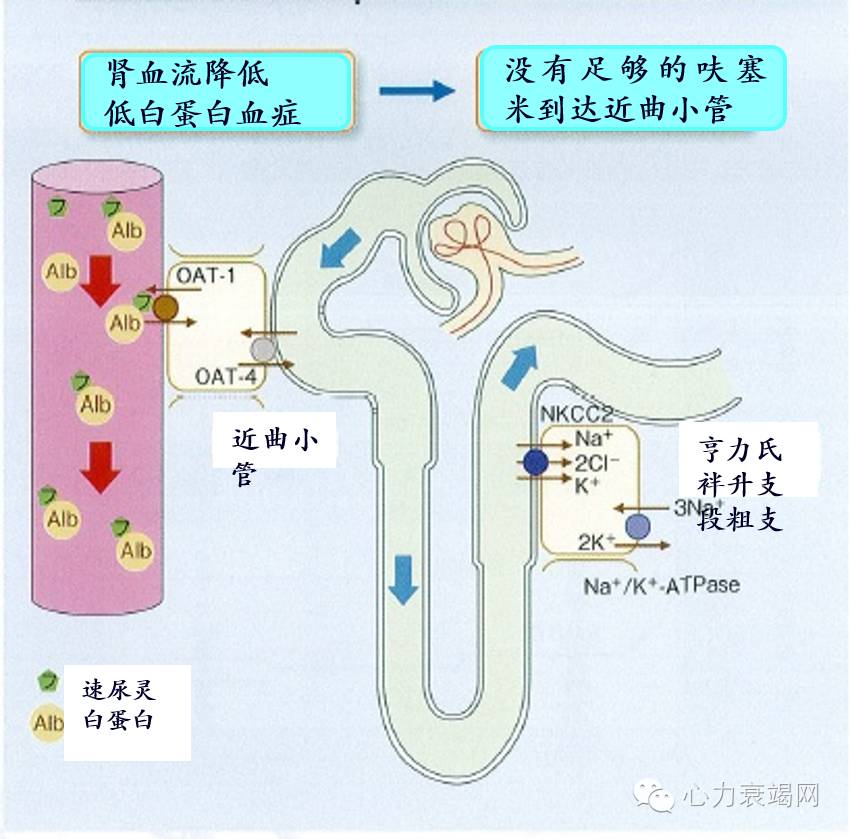
呋塞米的作用机制及影响因素
【影响袢利尿剂作用的因素】:
◆1.肾血流量下降
◆2.肾小球率过滤下降
◆3.低蛋白血症
◆4.蛋白尿
◆5.肾小管间质损害
◆6.醛固酮
◆7.某些药物(西咪替丁,NSAID)
◆8.肠道管腔浮肿
袢利尿剂呋塞米在血液中与白蛋白结合,转移至近端小管周围的毛细血管,在有机阴离子转运蛋白(OAT-1,OAT-4)作用下,被尿道腔内吸收后,与肾小球滤过液一同转移至汉勒氏袢升支粗段,从而阻碍Na+·K+·2Cl-协同转运蛋白(NKCC2),抑制Na的再吸收
【利尿剂的缺陷】:
◆1.激活神经内分泌系统
◆2.加重心衰进程
◆3.加重电解质紊乱
◆4.排Na+、排K+、排Ca2+、排Mg2+
◆5.增加心律失常导致的死亡率
◆6.减轻容量的效果不理想(利尿剂抵抗)
◆7.低钠时无效, 本身是导致低钠的原因
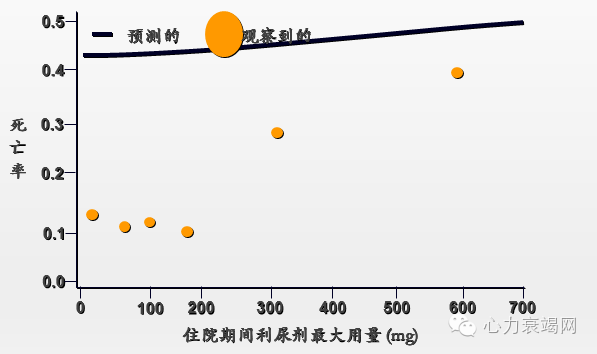
ESCAPE研究: 利尿剂剂量和死亡率关系
[4]
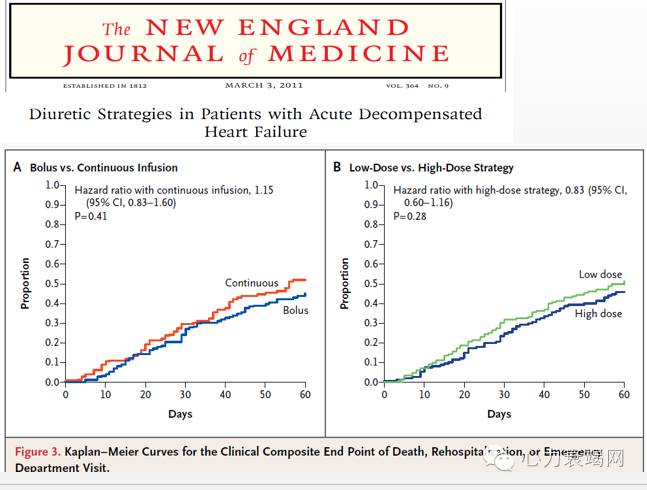
袢利尿剂对于急性失代偿性心衰患者可能具有致命的危害...
[5]
Exclusion criterion
Patients with SBP of less than 90 mm Hg or a serum creatinine level that was greater than 3.0 mg per deciliter (265.2 μmol per liter) and patients requiring intravenous vasodilators or inotropic agents (other than digoxin) for heart failure were excluded.
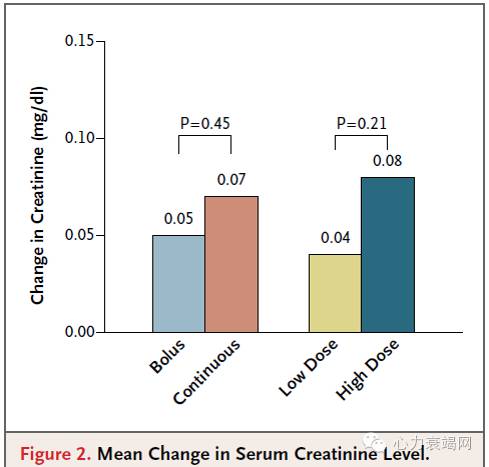
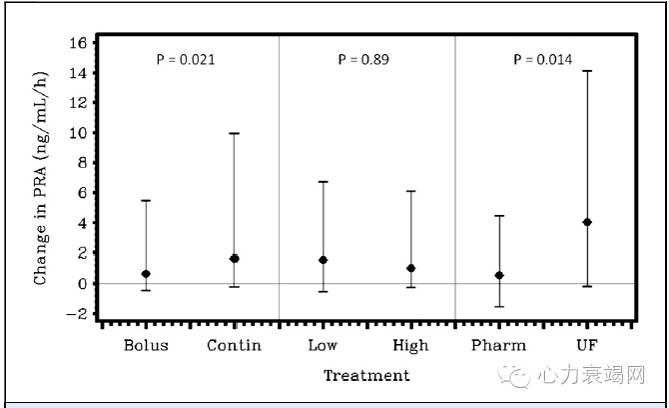
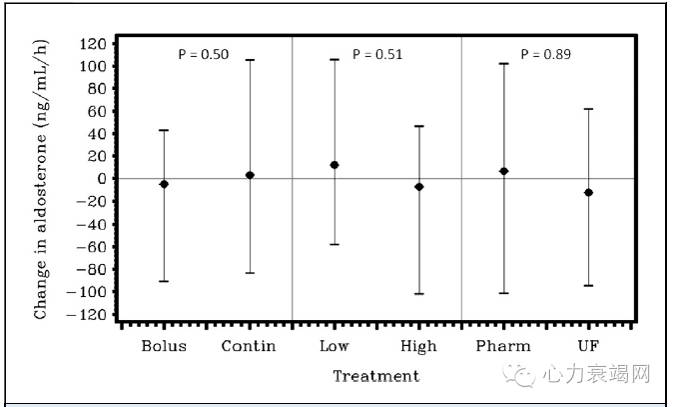
利尿剂使用策略与神经内分泌激活
[6]
PRA and Aldosterone Change From Baseline Based on Decongestion Strategy
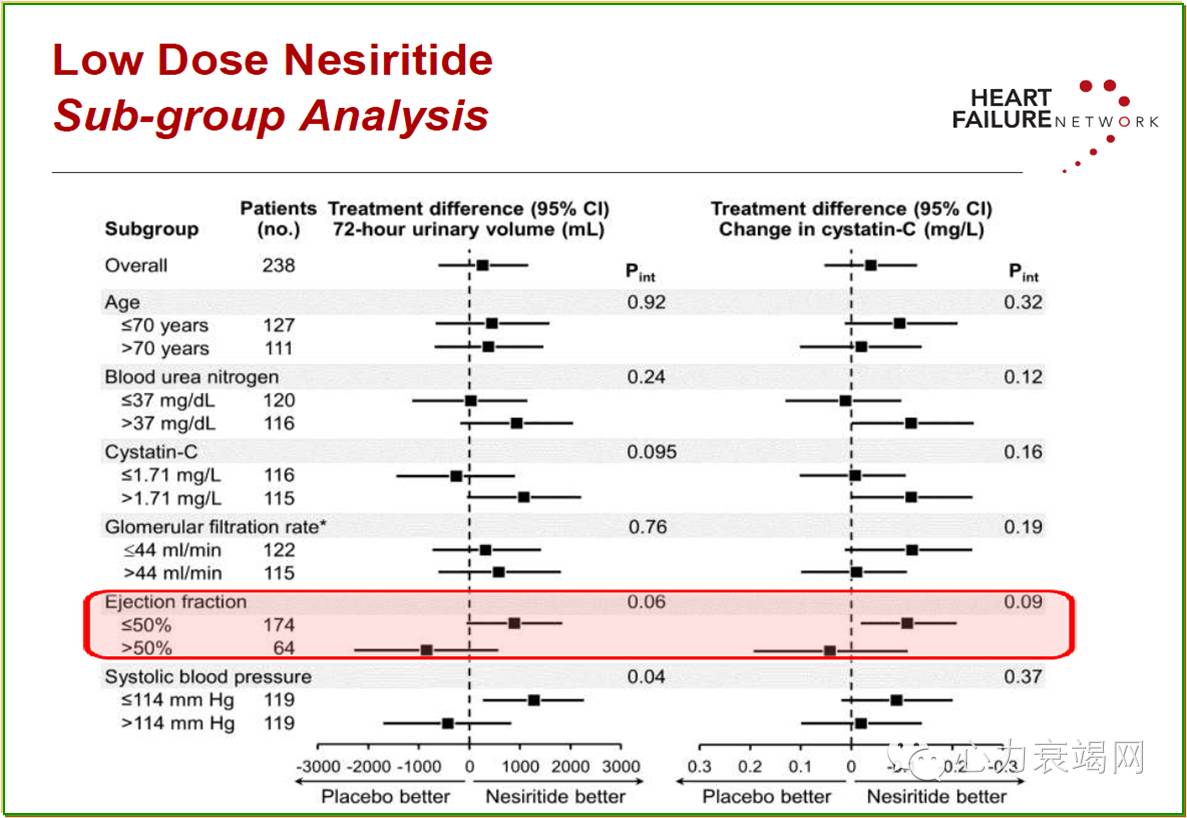
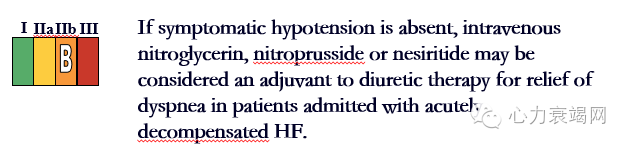
2、血管扩张剂
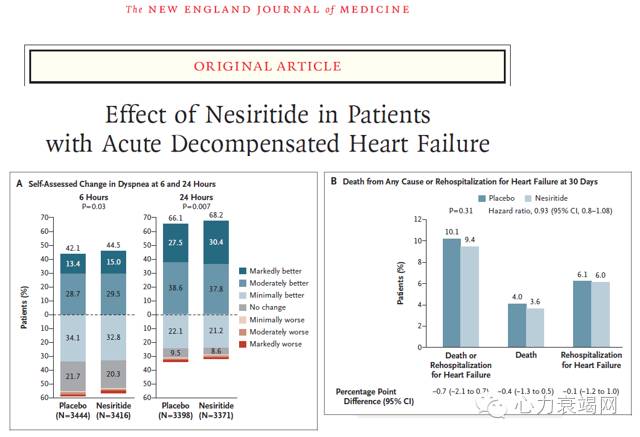
血管扩剂(奈西立肽)
新活素 (重组人脑利钠肽 rhBNP)
DNA基因重组技术、大肠杆菌为生产菌种制成的冻干粉针剂
32个氨基酸
分子量:3464 Da
与内源性脑利钠肽具有相同的氨基酸排序、空间结构和生物活性,因此具有相同的作用机制。
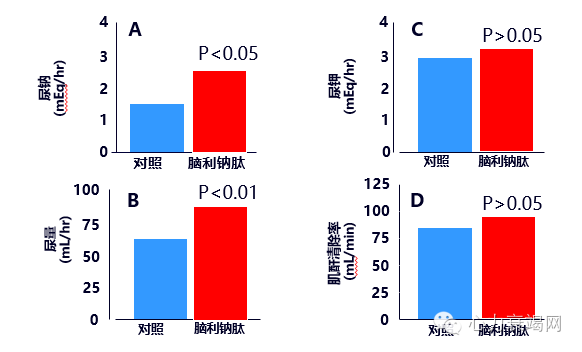
利钠排尿,对K+及SCr无影响
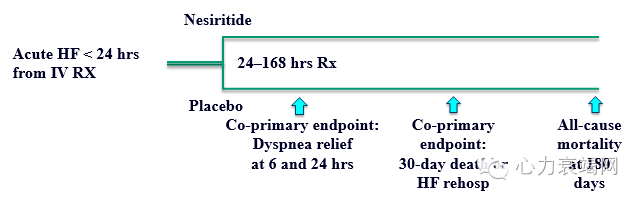
Study design and drug procedures
●Double – blind placebo controlled
●IV bolus (loading dose) of 2 µg/kg nesiritide or placebo
- Investigator’s discretion for bolus
- Followed by continuous IV infusion of nesiritide 0.01 µg/kg/min or placebo for up to 7 days
●Usual care per investigators including diuretics and/or other therapies as needed
●Duration of treatment per investigator based on clinical improvement
[7]
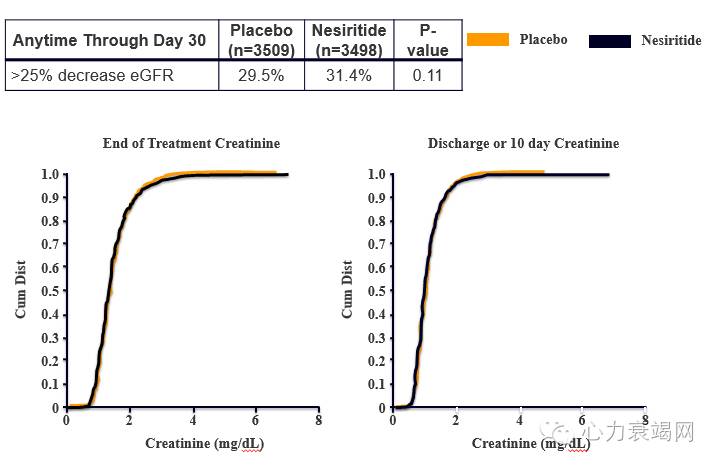
Renal Safety
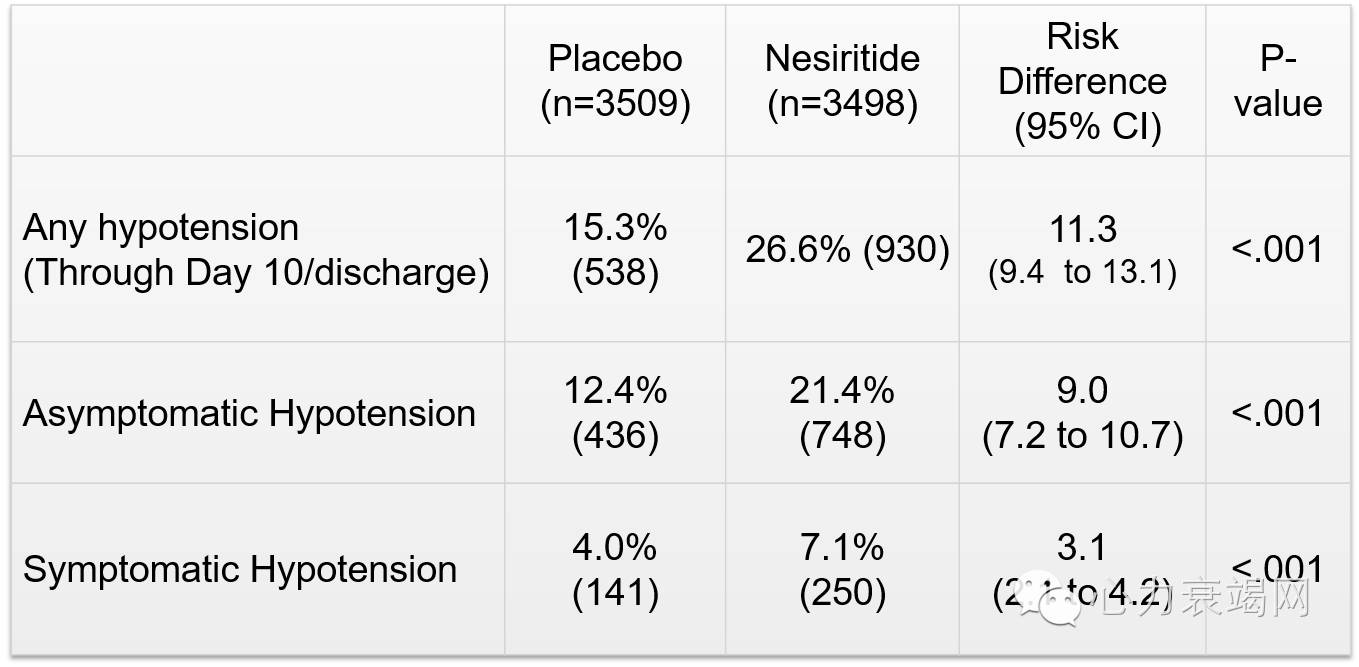
Hypotension
[8]
Parenteral Therapy in Hospitalized HF
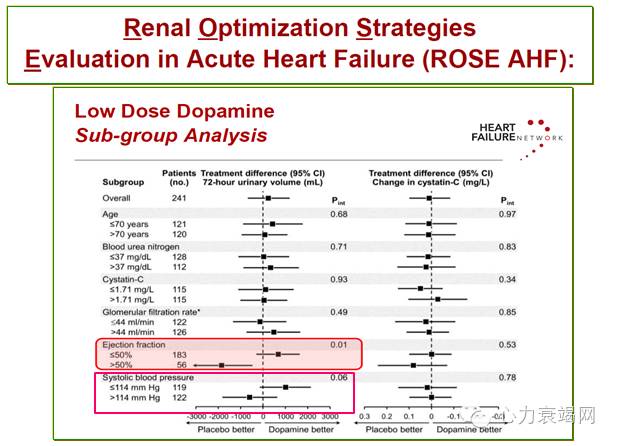
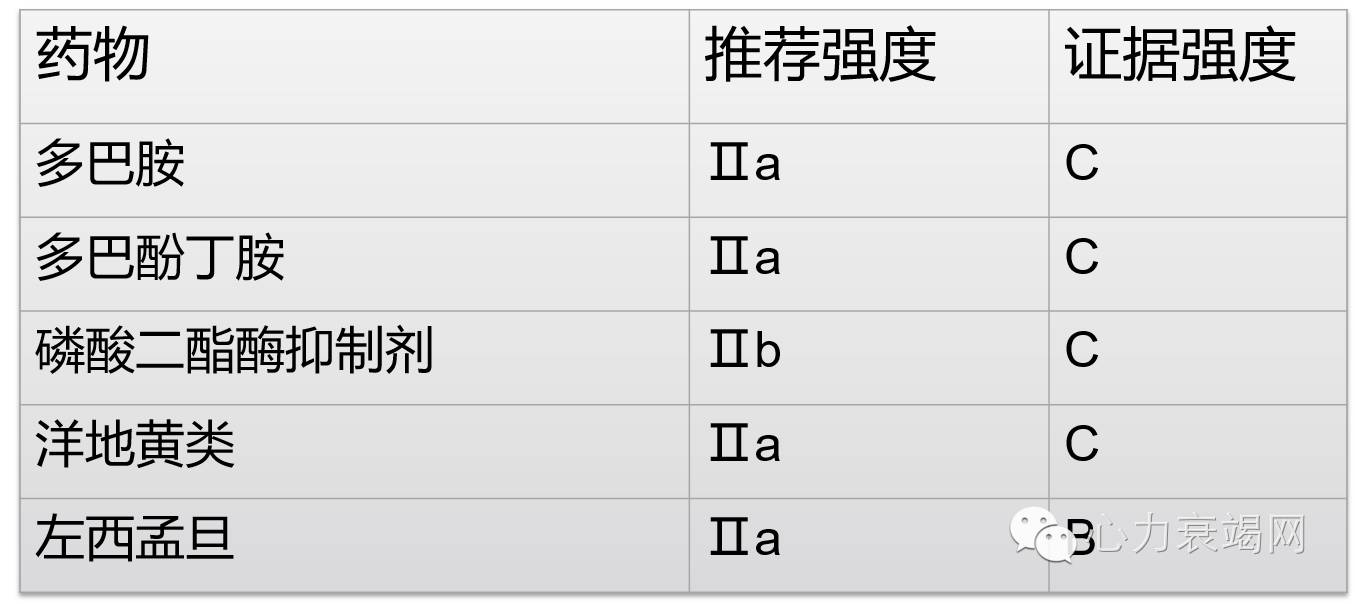
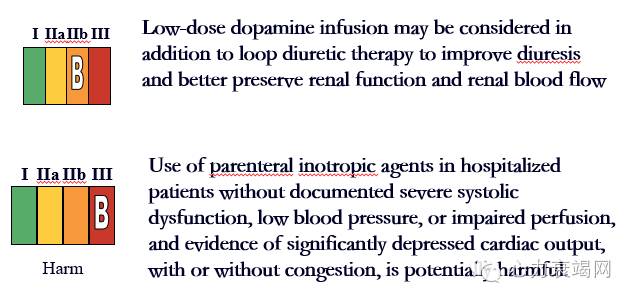
3、正性肌力药物
▶正性肌力药
-仅低血压和低排出时有效
Inotropic Support
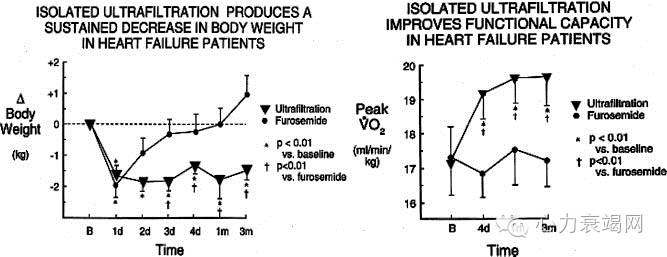
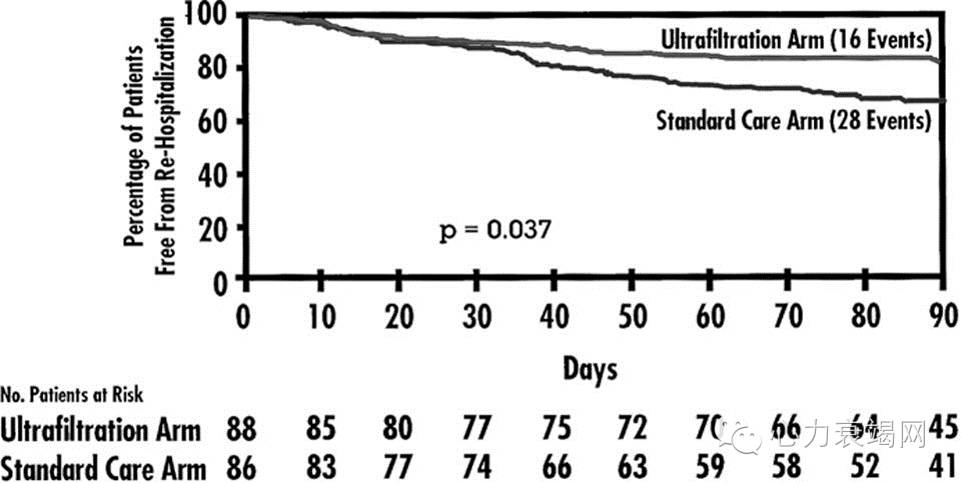
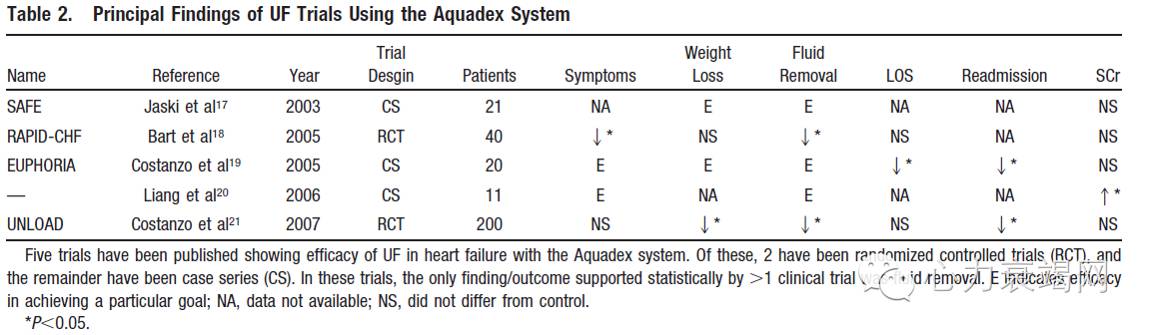
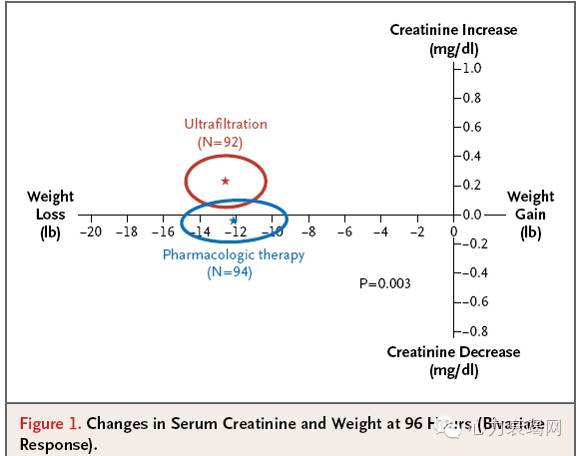
4、超滤
[9]
Sustained improvement in functional capacity after removal of body fluid with isolated ultrafiltration in chronic cardiac insufficiency:
failure of furosemide to provide the same result.
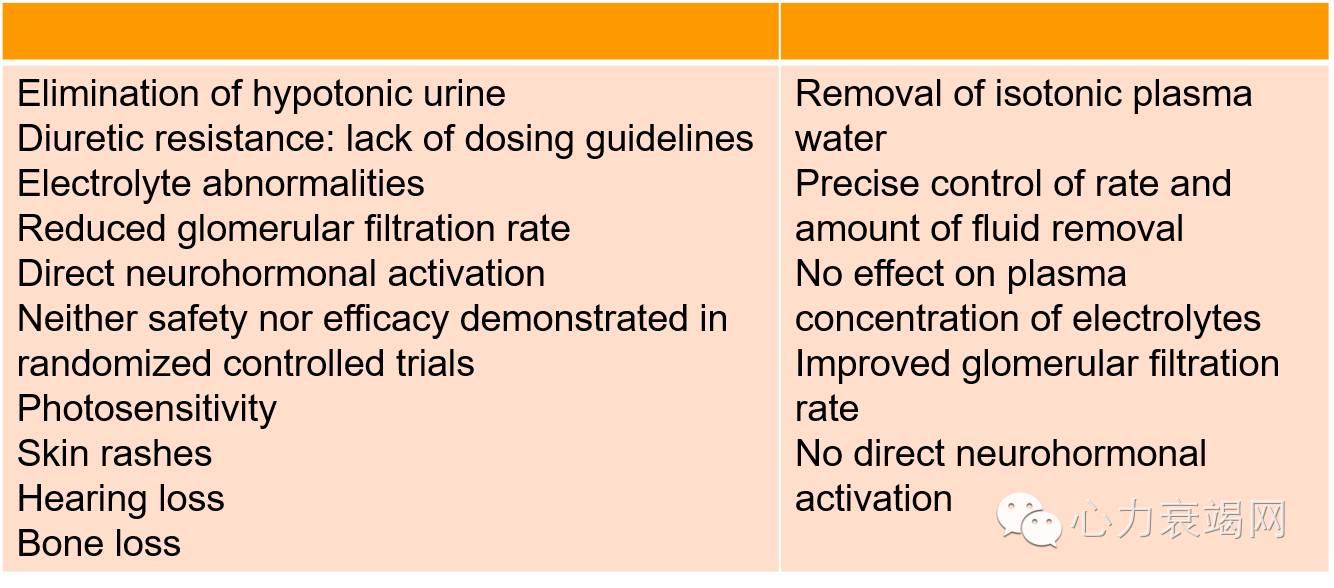
袢利尿剂的缺点与超滤
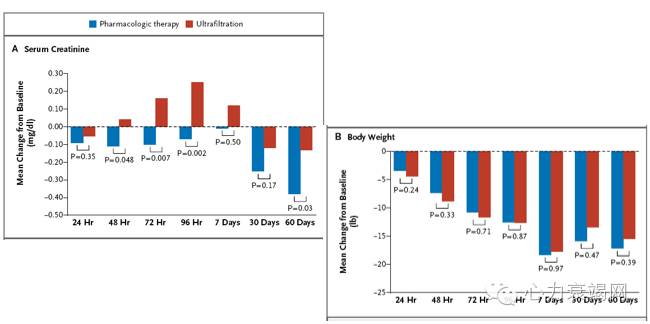
[10]
[11]
Changes from Baseline in Serum Creatinine and Body Weight at Various Time Points, According to Treatment Group.
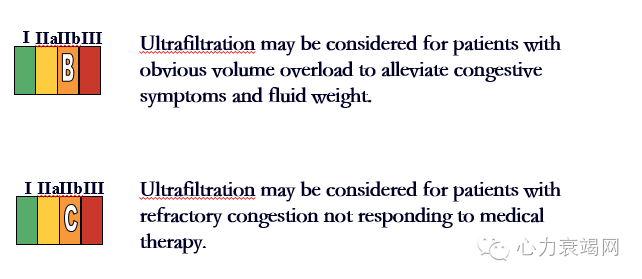
超滤
新型利尿剂提供新的方法
新型药物:托伐普坦

利尿药作用位点和分类
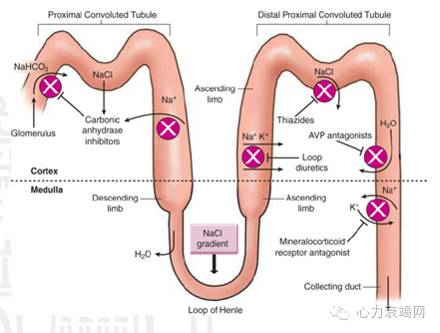
◆这是不同利尿剂在肾小管的作用位置,大多数作用在离子泵上,通过排钠排钾
◆只有醛固酮拮抗剂和托伐普坦是受体拮抗剂,新的指南已经将醛固酮拮抗剂从利尿剂中转划到神经激素受体拮抗剂
◆其实托伐普坦也兼具利尿和神经激素受体拮抗作用,只是目前它利尿的效果被更好证明。
心衰指南并未包括碳酸酐酶抑制剂
血管加压素AVP /抗利尿激素ADH
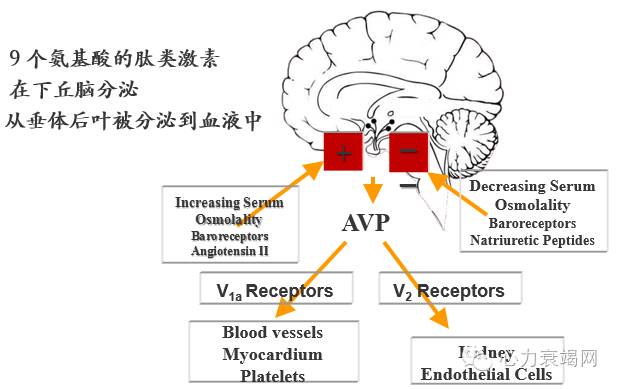
This slide shows you the basics about AVP stimulation and its effects. This is a complex topic, which we’ll summarize very briefly here. Basically, the control of vasopressin is dominantly under the control of the prevailing serum or plasma osmolality. That’s why, as you see on the left-hand side of the slide, hyperosmolality is the first stimulus for AVP secretion. This is a very tightly regulated system. Even a 1 milliosmole/kg increase in serum osmolality will trigger an increase in AVP secretion; it’s that important in terms of maintaining tonicity of the body fluids. There are other central stimuli, however. Volume depletion, hypotension, and central mediators such as angiotensin II are also linked to AVP secretion. In humans we know that hyperosmolality has evolved as the primary stimulus. Hypovolemia may or may not be involved until extreme hypotension occurs and there is indirect evidence that angiotensin II and other central mediators may also be involved in controlling AVP secretion. VAPRISOL is contraindicated in hypovolemic hyponatremia.
On the other side of the slide, you have some of the inhibitory influences on AVP. If hyperosmolality stimulates vasopressin, hypoosmolality inhibits it. We then have the role of various baroreceptors. Again, we’re not quite sure how important those are in humans, but when blood pressure rises, particularly to very high levels, it’s been demonstrated to at least modulate the osmotic secretion of AVP. And then there are some other neurohumoral factors such as the natriuretic peptides, which have been linked to suppressed AVP secretion in the same way that angiotensin II stimulates it.
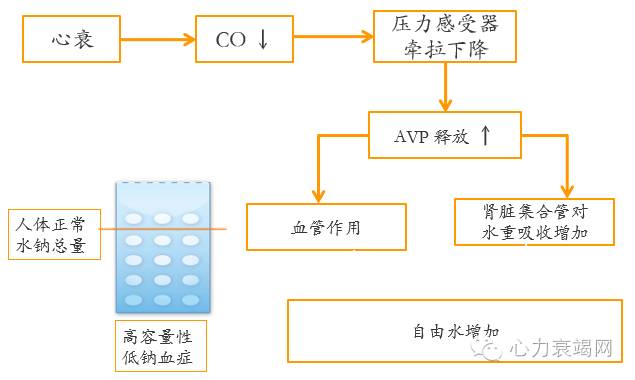
AVP在心衰的水潴留中扮演重要角色
心衰患者AVP升高 与严重程度相关
[12]
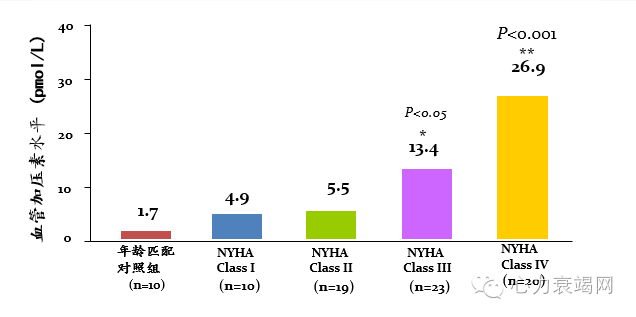
AVP在心衰患者中水平增高并非完全是一种理论推测, 而且是有证据的.
住院心衰病人低钠发生率
[13][14][15][16][17]
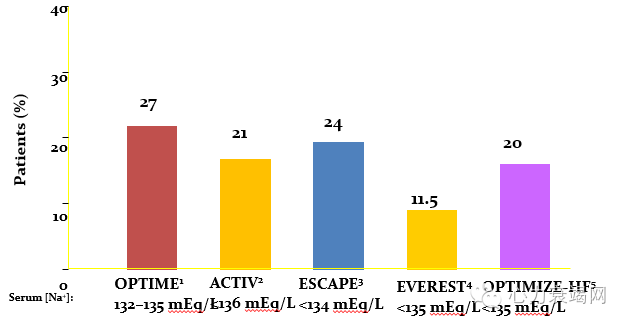
Hyponatremia is frequently present in patients hospitalized with acute decompensated heart failure (HF)
In the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study, 27% (256/943) of the patients hospitalized for worsening heart with systolic dysfunction had a serum [Na+] between 132 and 135 mEq/L1
In the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Congestive Heart Failure (ACTIV in CHF) trial, 21% (68/319) of patients hospitalized for HF with left ventricular ejection fraction (LVEF) <40% had a serum [Na+] <136 mEq/L2
In the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness (ESCAPE) trial, 24% (103/430) of patients hospitalized with New York Heart Association class IV HF with systolic dysfunction (LVEF <30%) had baseline serum [Na+] <134 mEq/L3
In the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) trial, 11.5% of patients hospitalized for HF with systolic dysfunction had a baseline serum [Na+] <135 mEq/L)4
Although inclusion and exclusion criteria may have influenced the prevalence of hyponatremia observed in these trials, these findings are supported by data from a large HF registry
In the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients With Heart Failure (OPTIMIZE-HF) registry, 20% (9368/47647) of patients hospitalized with new-onset or worsening HF, irrespective of systolic function, had baseline serum [Na+] <135 mEq/L5
Klein L et al. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study. Circulation. 2005;111(19):2454-2460.
Gheorghiade M et al. Effects of tolvaptan, a vasopressin antagonist, in patients hospitalized with worsening heart failure: a randomized controlled trial. JAMA. 2004;291(16):1963-1971.
Gheorghiade M et al. Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE trial. Arch Intern Med. 2007;167(18):1998-2005.
Data on file: Protocol 156-02-236. Otsuka America Pharmaceutical, Inc.
Gheorghiade M et al. Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE-HF registry. Eur Heart J. 2007;28(8):980-988.
[18]
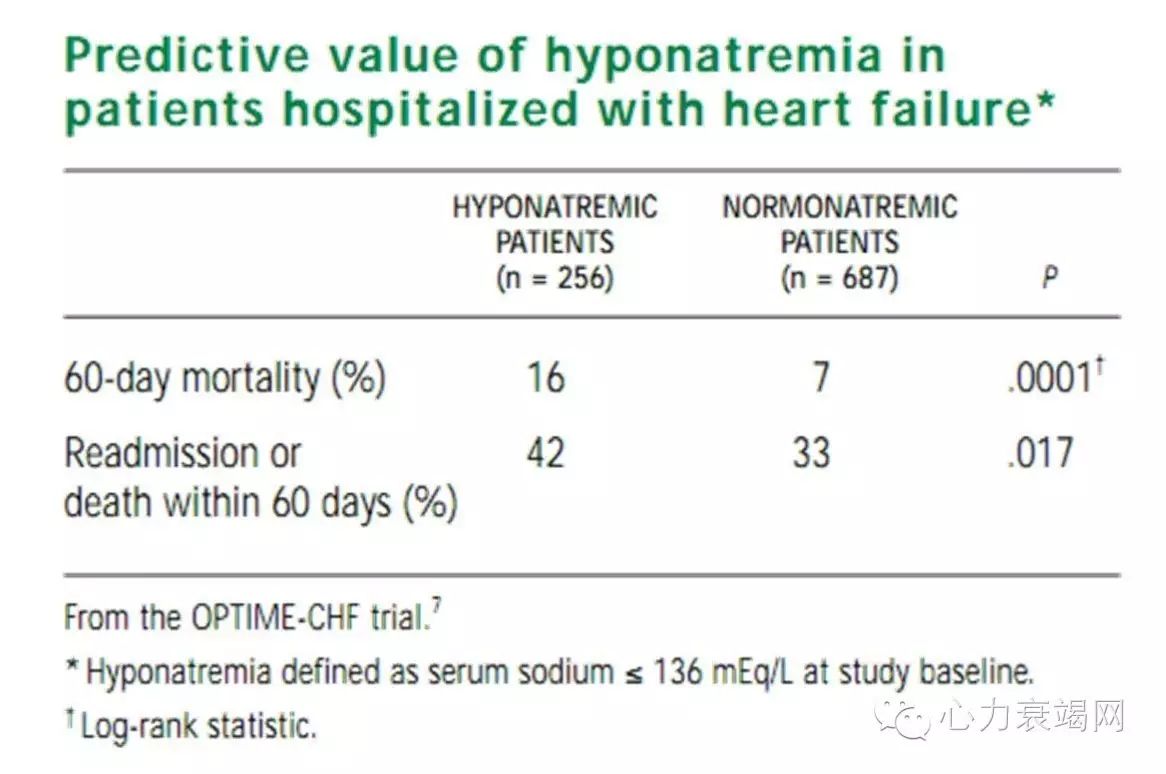
Among heart failure patients treated with angiotensin-converting enzyme (ACE)inhibitors, diuretics, and beta-blockers, even a small decline in serum sodium levels, to 136mEq/L or less, was associated with more than twice the risk of 60-day mortality and a significant increase in risk of readmission or death within 60 days compared with serum sodium levels greater than 136 mEq/L
【托伐普坦心衰领域主要临床试验】
◆1.ECLIPSE- 单剂量血流动力学
◆2.ACTIV – 急性心衰, 60天
◆3.METEOR – 慢性心衰, 52周
◆4.EVEREST – 急性心衰, 2+ 年
◆5.QUEST- 急性/慢性心衰, 14 天
◆6.对神经激素和肾 功能的影响

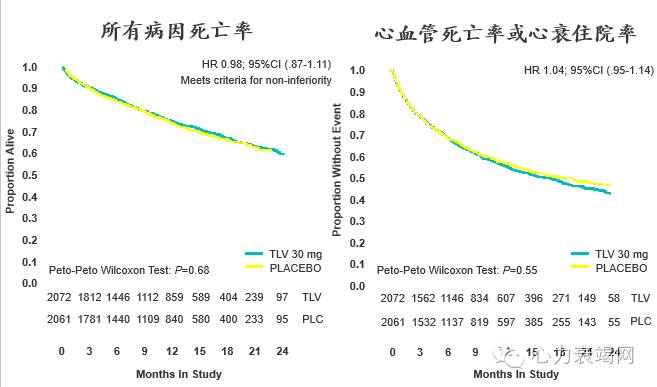
联合结局试验设计
[19]
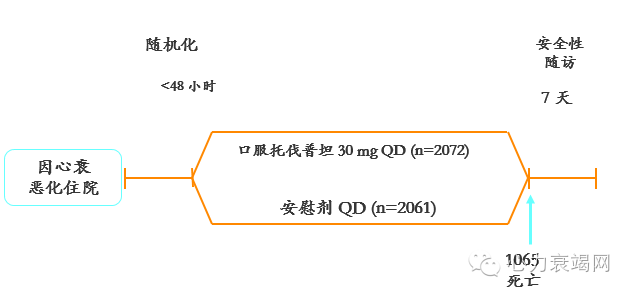
【双重主要终点】:
所有原因死亡率改善/非劣效性
心血管死亡或心衰住院改善
短期:苏麦卡®明显改善心衰症状
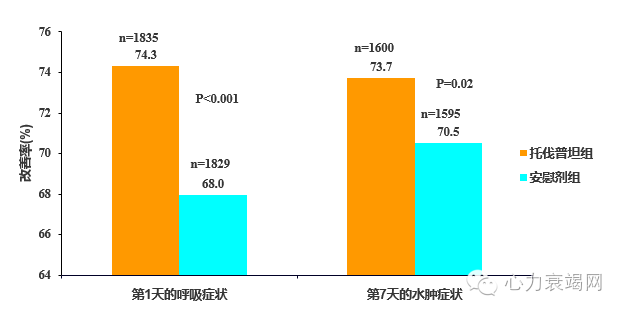
此图描述的是针对4133例心衰患者的EVERST试验,短期的试验表明苏麦卡在第一天时就能有效改善呼吸症状,效果显著强于对照组;第七天可以改善水肿症状,此试验很好的证明苏麦卡可明显改善心衰症状,也正是基于这个短期试验,苏麦卡目前已是2012年ESC指南推荐用于急性心衰的药物。
附注:2012年ESC心衰指南:2012欧洲心脏病学会(ESC)急慢性心力衰竭诊断和治疗指南。
参考文献:
18.Gheorghiade M,et al: Short-term Clinical Effects of Tolvaptan, an Oral Vasopressin Antagonist, in Patients Hospitalized for Heart Failure. JAMA.2007 Mar 28;297(12):1332-43. Epub2007,Mar25
长期总体结局
[20]
长期低钠亚组:有改善倾向
[21]
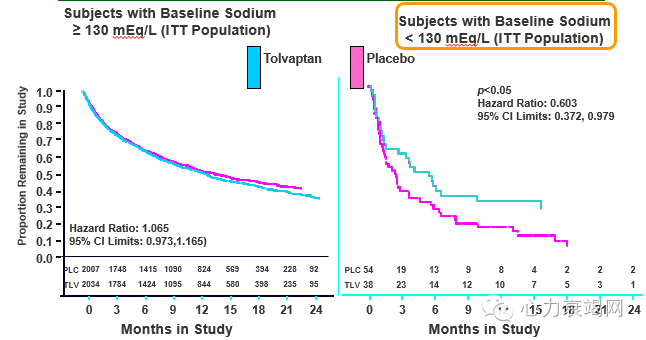
we observed essentially no separation in the curves in the subgroup of patients > 130, shown here on the left, but separation occurred as early as 2 months in the subgroup of patients with Na less than 130.
To be clear: This is a non- pre-specified post hac analysis to explore potentially supportive data…and it provides a further indication for the safety of tolvatan in this important sub-group of patients
*Pause on slide 2 seconds
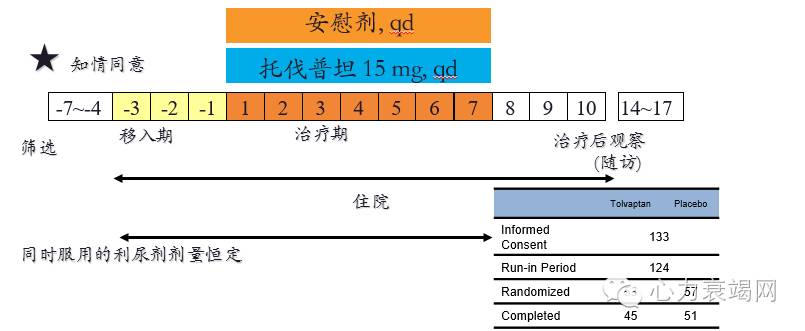
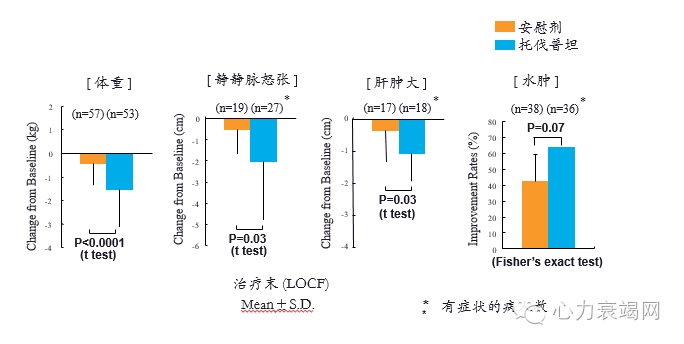
QUEST研究设计
多中心, 随机, 双盲, 安慰剂对照
加用, 同时服用的利尿剂剂量恒定
体重变化
[22]
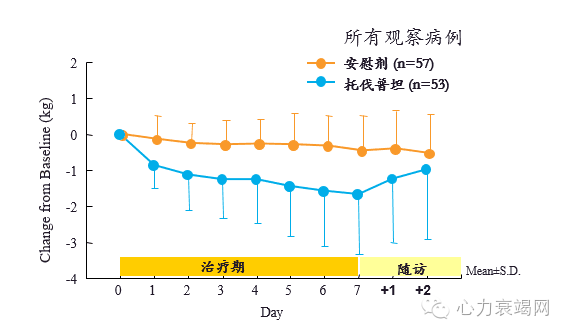
托伐普坦的有效性
[22]
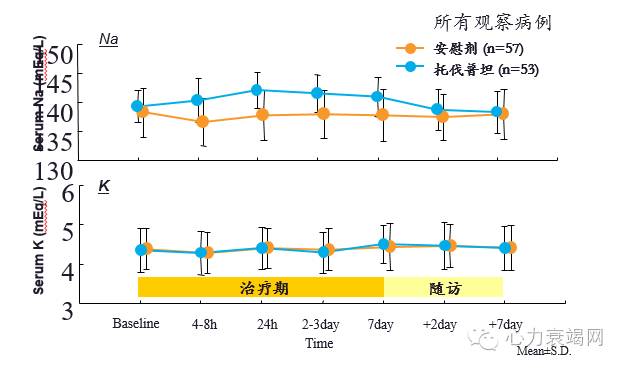
血清电解质
[22]
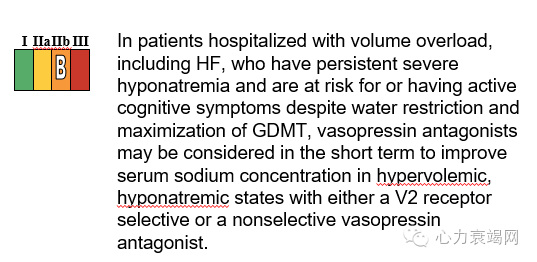
Arginine Vasopressin Antagonists
【心衰容量超负荷可选择的治疗策略】:
1.利尿剂
2.血管扩张剂
3.正性肌力药
4.超滤
5.新型药物:托伐普坦
小 结
1.心衰容量负荷增加与多种机制有关
2.处理个体化
2.新型利尿剂提供新的方法
参考文献:
★ [1]Drazner MH, Rame JE, Stevenson LW, Dries DL. Prognostic importance of elevated jugular venous pressure and a third heart sound in patients with heart failure. N Engl J Med 2001;345:574–581
[2]Chaudhry E al. Circulation 2007; 116: 1549-15
[3]Fonarow GC. Rev Cardiovasc Med. 2003;4(suppl 7):S21-S30
[4]Hasselblad V, et al. J Card Fail. 2005
[5]Felker, G. M. et al.: Circ. Heart Fail., 2(1), 56-62, 2009
[6]J Am Coll Cardiol HF 2015
[7]N Engl J Med 2011;365:32-43.
[8]JAMA. 2013 Dec 18;310(23):2533-43.
[9]Am J Med. 1994;96: 191–199. J Am Coll Cardiol. 2007;49:675– 683
[10]Circ Heart Fail. 2009;2:505-511
[11]N Engl J Med 2012;367:2296-304. DOI: 10.1056/NEJMoa1210357
[12]Data from 72 subjects with CHF admitted to Omiya Medical Center in Japan.
Nakamura T et al. Int J Card. 2006;106(2):191-195.
[13]Klein L et al. Circulation. 2005;111(19):2454-2460;
[14] Gheorghiade M et al. JAMA. 2004;291(16):1963-1971;
[15]Gheorghiade M et al. Arch Intern Med. 2007;167(18):1998-2005;
[16]Data on file: Protocol 156-02-236;
[17] Gheorghiade M et al. Eur Heart J. 2007;28(8):980-988.
[18]J Card Fail 2003; 9:S83. Abstract.
[19]Gheorghiade, et al. J Card Fail. 2005;11:260-269.
[20]Konstam et al. JAMA 2007
[21]Overall CV Mortality/Morbidity (ITT) HR 1.04; 95%CI (.95-1.14)
[22]Circ J 73 (Suppl.1): 127,2009★
男,主任医师,教授,博士生导师。毕业于山东省滨州医学院。1996年毕业于原上海医科大学研究生院并获心血管专业博士学位。1999~2000年国家留学基金委公派赴德访问学者。现为复旦大学附属中山医院、上海市心血管病研究所心内科硕士生导师,上海心脏起搏与电生理学会会员,中华医学会会员,主要从事各种心血管疾病的研究和临床工作。
临床主要从事心律失常,心力衰竭,冠心病,高血压等疾病的诊疗和科研工作,特别是各种类型的快速心律失常的经导管射频消融治疗,包括室上性心动过速、房性心动过速、心房扑动、心房颤动、室性心动过速等。其中心房颤动和室性心动过速的射频消融处于国内领先地位。先后主持国家自然科学基金、教育部等科研基金课题项,参加国家“十五”攻关课题研究。在国内外杂志发表论文50余篇,参与编写大型教材和参考书籍多本。